


According to the U.S. Centers for Disease Control, one out of every three adults in the United States have prediabetes, a condition marked by elevated blood sugar levels that could lead to the development of type 2 diabetes. The good news is that, if detected early, prediabetes can be reversed through lifestyle changes such as improved diet and exercise. The bad news? Eight out of 10 Americans with prediabetes don’t know that they have it, putting them at increased risk of developing diabetes as well as disease complications that include heart disease, kidney failure and vision loss.
Current screening methods typically involve a visit to a health care facility for laboratory testing and/or the use of a portable glucometer for at-home testing, meaning access and cost may be barriers to more widespread screening. But researchers at the University of Washington’s Paul G. Allen School of Computer Science & Engineering and UW Medicine may have found the sweet spot when it comes to increasing early detection of prediabetes. They developed GlucoScreen, a new system that leverages the capacitive touch sensing capabilities of any smartphone to measure blood glucose levels without the need for a separate reader. Their approach will make glucose testing less costly and more accessible — particularly for one-time screening of a large population.
The team describes GlucoScreen in a new paper published in the latest issue of the Proceedings of the Association for Computing Machinery on Interactive, Mobile, Wearable and Ubiquitous Technologies (IMWUT).
“In conventional screening, a person applies a drop of blood to a test strip, where the blood reacts chemically with the enzymes on the strip. A glucometer is used to analyze that reaction and deliver a blood glucose reading,” explained lead author Anandghan Waghmare, a Ph.D. student in the Allen School’s UbiComp Lab. “We took the same test strip and added inexpensive circuitry that communicates data generated by that reaction to any smartphone through simulated tapping on the screen. GlucoScreen then processes the data and displays the result right on the phone, alerting the person if they are at risk so they know to follow up with their physician.”
The GlucoScreen test strip samples the electrochemical reaction induced by the mixing of blood and enzymes as an amplitude along a curve at a rate of five times per second. The strip transmits this curve data to the phone encoded in a series of touches at variable speeds using a technique called pulse width modulation. “Pulse width” refers to the distance between peaks in the signal — in this case, the length between taps. Each pulse width represents a value along the curve; the greater the distance between taps for a particular value, the higher the amplitude associated with the electrochemical reaction on the strip.

“You communicate with your phone by tapping the screen with your finger,” said Waghmare. “That’s basically what the strip is doing, only instead of a single tap to produce a single action, it’s doing multiple taps at varying speeds. It’s comparable to how Morse code transmits information through tapping patterns.”
The advantage of this technique is that it does not require complicated electronic components, which minimizes the cost to manufacture the strip and the power required for it to operate compared to more conventional communication methods like Bluetooth and WiFi. All of the data processing and computation occurs on the phone, which simplifies the strip and further reduces the cost.
“The test strip doesn’t require batteries or a USB connection,” noted co-author Farshid Salemi Parizi, a former Ph.D. student in the UW Department of Electrical & Computer Engineering who is now a senior machine learning engineer at OctoML. “Instead, we incorporated photodiodes into our design so that the strip can draw what little power it needs for operation from the phone’s flash.”
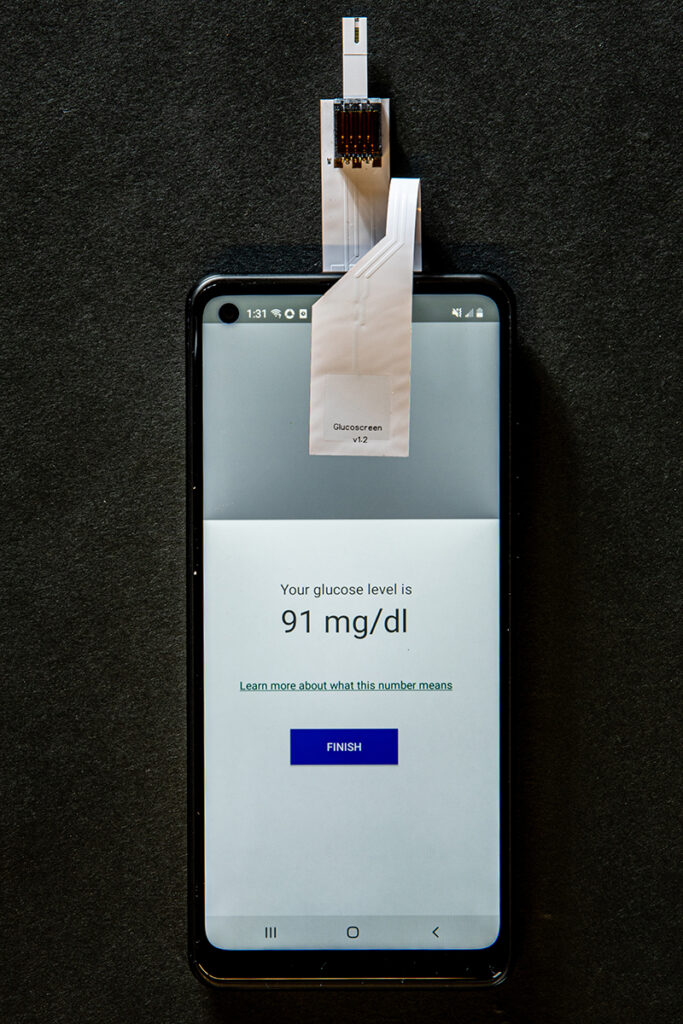
The flash is automatically engaged by the GlucoScreen app, which walks the user through each step of the testing process. First, a user affixes each end of the test strip to the front and back of the phone as directed. Next, they prick their finger with a lancet, as they would in a conventional test, and apply a drop of blood to the biosensor attached to the test strip. After the data is transmitted from the strip to the phone, the app applies machine learning to analyze the data and calculate a blood glucose reading.
That stage of the process is similar to that performed on a commercial glucometer. What sets GlucoScreen apart, in addition to its novel touch technique, is its universality.
“Because we use the built-in capacitive touch screen that’s present in every smartphone, our solution can be easily adapted for widespread use. Additionally, our approach does not require low-level access to the capacitive touch data, so you don’t have to access the operating system to make GlucoScreen work.” explained co-author Jason Hoffman, a Ph.D. student in the Allen School. “We’ve designed it to be ‘plug and play.’ You don’t need to root the phone — in fact, you don’t need to do anything with the phone, other than install the app. Whatever model you have, it will work off the shelf.”
Hoffman and his colleagues evaluated their approach using a combination of in vitro and clinical testing. Due to the COVID-19 pandemic, they had to delay the latter until 2021 when, on a trip home to India, Waghmare connected with Dr. Shailesh Pitale at Dew Medicare and Trinity Hospital. Upon learning about the UW project, Dr. Pitale agreed to facilitate a clinical study involving 75 consenting patients who were already scheduled to have blood drawn for a laboratory blood glucose test. Using that laboratory test as the ground truth, Waghmare and the team evaluated GlucoScreen’s performance against that of a conventional strip and glucometer.
While the researchers stress that additional testing is needed, their early results suggest GlucoScreen’s accuracy is comparable to that of glucometer testing. Importantly, the system was shown to be accurate at the crucial threshold between a normal blood glucose level at or below 99 mg/dL, and prediabetes, defined as a blood glucose level between 100 and 125 mg/dL. Given the scarcity of training data they had to work with for the clinical testing model, the researchers posit that GlucoScreen’s performance will improve with more inputs.
According to co-author Dr. Matthew Thompson, given how common prediabetes as well as diabetes are globally, this type of technology has the potential to change clinical care.
“One of the barriers I see in my clinical practice is that many patients can’t afford to test themselves, as glucometers and their test strips are too expensive. And, it’s usually the people who most need their glucose tested who face the biggest barriers,” said Thompson, a family physician and professor in the UW Department of Family Medicine and Department of Global Health. “Given how many of my patients use smartphones now, a system like GlucoScreen could really transform our ability to screen and monitor people with prediabetes and even diabetes.”
GlucoScreen is presently a research prototype; additional user-focused and clinical studies, along with alterations to how test strips are manufactured and packaged, would be required before the system could be made widely available. According to senior author Shwetak Patel, the Washington Research Foundation Entrepreneurship Endowed Professor in Computer Science & Engineering and Electrical & Computer Engineering at the UW, the project demonstrates how we have only begun to tap into the potential of smartphones as a health screening tool.
“Now that we’ve shown we can build electrochemical assays that can work with a smartphone instead of a dedicated reader, you can imagine extending this approach to expand screening for other conditions,” Patel said.
Yuntao Wang, a research professor at Tsinghua University and former visiting professor at the Allen School, is also a co-author of the paper. This research was funded in part by the Bill & Melinda Gates Foundation.